

Table of contents
If you’ve ever looked at an operative note, a CPT update, and a payer denial explanation all at once and wondered, “How did billing get this complicated?”, you’re looking at the new economics of orthopedic billing.
The rules changed quietly. The financial impact didn’t.
The orthopedic coding errors are no longer isolated billing issues. CMS reimbursement cuts, CPT coding changes, AI-driven payer audits, and tighter documentation requirements are creating a financial environment where small billing mistakes now carry outsized consequences for orthopedic practices.
The average coding-related claim denial dollar amount rose 126% in 2024, from $297 to $631 per denial.
Today, coding errors don’t just create occasional denials. They create recurring revenue leakage across high-volume orthopedic procedures, especially when payer AI tools identify the same documentation or modifier pattern repeatedly.
Which means what looks like a small coding inconsistency inside the billing department can eventually become a six-figure reimbursement problem for the practice.
And because orthopedic EBITDA multiples remain high, every dollar lost to preventable orthopedic coding errors carries a much larger enterprise value impact behind it.
Why Are Orthopedic Coding Errors Increasing Revenue Risk in 2026?
If you’ve ever watched a clean surgical case turn into a 90-day denial chase, you already know something is broken. You just might be looking for it in the wrong place.
Ask most practice leaders where orthopedic coding errors live in their organization and they’ll point you to the billing team. That’s where denials get worked. That’s where claims get resubmitted. That’s where the problem gets handled.
And that’s exactly why the problem keeps getting bigger.
That framing is expensive. In 2026, a single modifier error on a high-volume procedure code isn’t just a denied claim. It’s a pattern that payer AI tools can now identify across 24 months of similar submissions and audit retroactively. By the time your billing team catches it, the exposure is already built.
A documentation gap in a rotator cuff repair operative note isn’t just a resubmission. It’s consistent downcoding across every similar case your practice bills, until someone goes back and fixes the template that created it.
And a billing team that hasn’t updated its workflows for the 2026 CPT code changes isn’t just slow to adapt. It’s generating revenue risk on every single claim it touches.
The billing team isn’t where your coding problem ends. It’s where your coding problem surfaces. The difference matters, because one is a workflow fix, and the other is a revenue strategy.
According to the Experian Health State of Claims 2025 Report, 41% of U.S. healthcare providers now report denial rates at or above 10%. That’s not a compliance trend. That’s a margin trend. And orthopedics sits at the center of it.
Get a Free Orthopedic Billing Audit to identify denial patterns, underpayments, and CPT-level revenue risks affecting your practice.
What Changed in Orthopedic Billing in 2026?
Most practices felt the shift in January. Not all of them understood why.
Here’s what actually changed, and what it’s costing you.
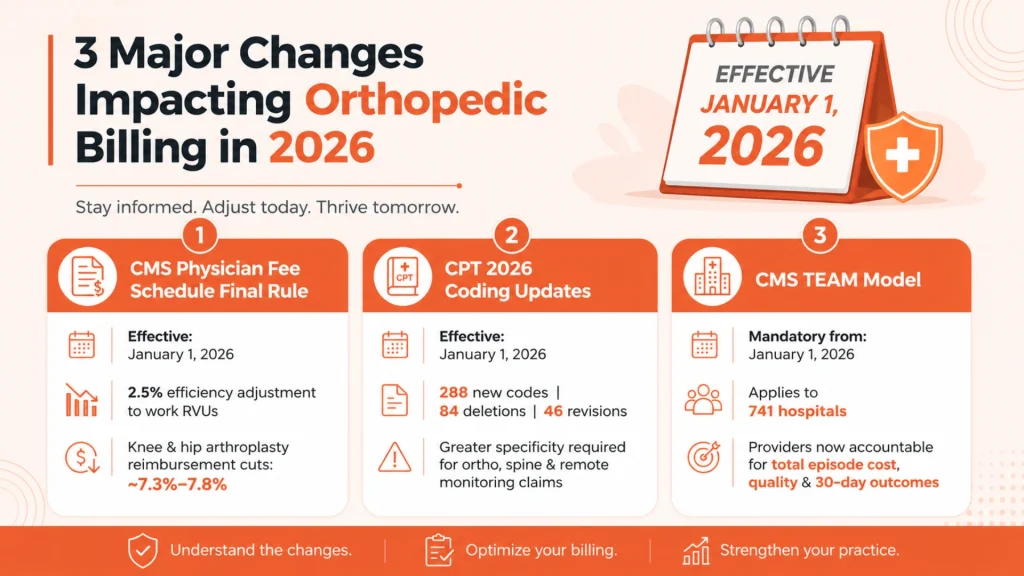
CMS Physician Fee Schedule Final Rule Built a Pay Cut Into the Math
The CY 2026 Physician Fee Schedule Final Rule didn’t arrive with a headline that said “we’re reducing your reimbursement.” It arrived with language about efficiency.
CMS finalized a −2.5% efficiency adjustment on the intraservice time component of work RVUs across all non-time-based procedures. The technology and workflow improvements have made procedures faster, so payment should reflect that.
The American Medical Association (AMA) publicly called the assumption flawed, relying on subjective survey data that penalizes procedural specialties for clinical advances that actually require more complexity, not less. But the rule passed anyway.
What that looks like in dollars:
The American Association of Hip and Knee Surgeons (AAHKS) ran the numbers on two of the highest-volume procedures in orthopedics:
- Total knee arthroplasty (CPT 27447): rate reduction of 7.3%–7.8%
- Total hip arthroplasty (CPT 27130): rate reduction of 7.3%–7.8%
For an orthopedic group with $5M in Medicare-allowable surgical charges, the 2.5% efficiency compression alone translates to $125,000 in reduced reimbursement, before a single denial is factored in.
2026 CPT Coding Changes Affecting Orthopedics
At the same time, the AMA’s CPT 2026 code set introduced:
- 288 new codes
- 84 deletions
- 46 revisions
- 418 total changes
Musculoskeletal, spine, and remote monitoring services were among the most affected, all requiring greater coding specificity than the year before.
Practices that didn’t update their orthopedic billing workflows at the start of the year aren’t just behind. They’re generating compounding revenue risk on every claim they touch, right now, today.
CMS TEAM Model Changes Orthopedic Revenue Risk
Then there’s the CMS TEAM Model (Transforming Episode Accountability Model), which became mandatory on January 1, 2026, for 741 acute care hospitals across selected regions.
Under TEAM, providers are financially accountable for:
- Total episode costs
- Care coordination quality
- Outcomes from surgery through 30 days post-discharge
For orthopedic groups affiliated with TEAM hospitals, this changes the stakes on coding accuracy. An upstream documentation gap doesn’t just affect one claim anymore. It has downstream financial consequences across an entire episode of care.
These three simultaneous shifts such as a structural reimbursement cut, a sweeping code set overhaul, and a mandatory new payment model; all landing on orthopedic practices that were built for a quieter environment.
Most mid-size and large groups are managing all of it with orthopedic billing workflows designed before any of it existed.
That’s not a billing problem. That’s a revenue strategy problem.
5 High-Risk Orthopedic CPT Codes That Are Draining Revenue
Orthopedic revenue leakage doesn’t spread evenly. It concentrates in predictable, high-volume code categories. Here’s where the most preventable losses live.
- Total Joint Arthroplasty (CPT 27447 & 27130)
What changed: The 2026 update revised the clinical distinction between partial and complete revision. Payers are now applying that distinction aggressively at adjudication.
What’s required now: Operative notes must explicitly document which components were addressed, the condition of existing hardware, and clinical rationale for the scope of revision.
Revenue risk: Incomplete notes don’t generate denials, they generate clean underpayments. For a program doing 300+ revision cases annually, systematic underpayment on 40% of those cases compounds into a six-figure invisible revenue gap. It won’t appear on your denial dashboard.
- Shoulder Arthroscopy (CPT 29827, 29807, 29822, 29823)
What changed: Payers now enforce a strict documentation hierarchy across these four codes. If the operative note doesn’t support the higher-specificity code, the claim drops to the nearest defensible code below it, automatically.
What’s required now: CPT 29827 and 29807 require explicit documentation of tear pattern, repair technique, suture anchor count, and lesion classification. Every element. Every case.
Revenue risk: The reimbursement gap between 29827 and 29822 exceeds $800 per case. On 400 shoulder arthroscopy cases annually with a 30% incomplete documentation rate, that’s a $96,000 annual gap, no denials, no flags, no AR report pointing back to it.
- Spinal Fusion & Decompression – CPT 22612, 22630, 63047
What changed: The 2026 revision tightened documentation requirements for multi-level fusion and introduced stricter interbody technique specificity. NCCI edit exposure increased across all multi-level cases.
What’s required now:
- 22612: Add-on code sequencing for additional levels must account for bilateral modifier (RT/LT) interactions and pre-2026 templates don’t handle this
- 22630: TLIF and PLIF must be explicitly differentiated in the operative note
- 63047: Decompression scope must be tied directly to specific nerve root pathology, not implied
Revenue risk: This is the only code category where you can overcode and undercode simultaneously, overcoding creates 24-month retroactive audit liability; undercoding leaves earned revenue uncollected. Both are happening, often across different providers in the same group.
- Joint Injections & Ultrasound Guidance (CPT 20610 & 76942)
What changed: Both codes received anatomical site-specific guidance revisions in 2026. Generic site documentation and generic guidance code application, both common practice before 2026, are now denial triggers.
What’s required now: Anatomical site must be documented with specificity, not category. Guidance code selection must match the specific site being imaged, not just the procedure being guided.
Revenue risk: On 1,200 injection visits annually, a 20% error rate generates denial or underpayment exposure on 240 claims per year, from a workflow problem that takes one afternoon to fix.
High-Risk Orthopedic CPT Codes: Where Revenue Leakage Concentrates
| CPT Code | Procedure | 2026 Risk Factor | Common Error |
|---|---|---|---|
| 27447 | Total Knee Arthroplasty | –7.3% to –7.8% CMS rate cut | Partial vs. complete revision miscoded; missing implant details in operative note |
| 27130 | Total Hip Arthroplasty | –7.3% to –7.8% CMS rate cut | Incomplete documentation of surgical approach and hardware condition |
| 29827 | Rotator Cuff Repair, Arthroscopic | High payer scrutiny | Missing tear pattern, repair technique, and suture anchor count in note |
| 29807 | SLAP Repair Arthroscopic | Frequently denied | Insufficient documentation of lesion classification and repair method |
| 29822 | Shoulder Arthroscopy, Limited Debridement | Downcode target | Miscoded from 29827 when operative note lacks specificity |
| 29823 | Shoulder Arthroscopy, Extensive Debridement | Downcode target | Confused with 29822; reimbursement gap between the two is significant |
| 20610 | Aspiration/Injection, Major Joint | High denial volume | Missing anatomical site documentation; wrong ultrasound guidance code paired |
| 76942 | Ultrasound Guidance for Injection | Revised 2026 guidance | Wrong code applied to anatomical site; incomplete imaging documentation |
| 27750 | Closed Tx, Tibial Shaft Fracture | 90-day global period risk | Missing manipulation technique, pre/post displacement degree, immobilization method |
| 22612 | Lumbar Fusion, Posterior | NCCI edit exposure | Incorrect add-on code sequencing on multi-level cases |
| 22630 | Lumbar Fusion, Posterior Interbody | Multi-level complexity | Bilateral modifier RT/LT interaction errors with add-on codes |
| 63047 | Lumbar Laminectomy with Facetectomy | High audit frequency | Insufficient documentation of nerve root involvement and decompression scope |
- Fracture Care (CPT 27750 & Global Period Management)
What changed: The 2026 documentation standard for initial fracture care encounters tightened. Payers are denying manipulation claims at elevated rates when notes lack required elements.
What’s required now: Every fracture care note must explicitly document manipulation technique, pre- and post-manipulation displacement degree, and immobilization method, all three, every time.
Revenue risk: The global period leaks from both ends. Billing a follow-up E/M inside the 90-day window is a compliance exposure payer AI tools are actively flagging. Missing billable services genuinely outside the global period is an equally common revenue leak, just quieter.
“The standardization of CPT codes has greatly streamlined billing, coding, and reimbursement – however, at the same time, it has harmed the same process by not allowing for grading of complexity.” Said Dr. Richard Yoon, MD, Director of Orthopedic Research and Division of Orthopedic Trauma and Adult Reconstruction Surgery at Jersey City Medical Center
The Most Common Modifier Errors in Orthopedic Billing
Modifier errors aren’t one-off mistakes. They live in billing templates, which means every claim that runs through that template carries the same error. That’s what turns a single workflow gap into a systematic revenue problem.
Here’s where the exposure concentrates.
- Modifier 51 – Multiple Procedures
The rule: Modifier 51 applies to secondary and subsequent procedures — not the highest-RVU code.
The error: Practices sequence it incorrectly, and the multiple procedure reduction hits the wrong claim.
The result: Consistent underpayment across every multi-procedure case — not a denial, a clean underpayment that processes without flagging.
Revenue risk: At 1,500+ surgical cases per year, one modifier sequencing error in a template is a six-figure annual problem.
Reduce Orthopedic Claim Denials Before They Affect Revenue
Billing workflow gaps, modifier errors, and documentation inconsistencies often create recurring reimbursement losses across orthopedic practices. See where your orthopedic revenue cycle may be leaking revenue.
- Modifier 59 & the X-Modifiers (XE, XS, XP, XU)
The rule: Required when a distinct procedural service is performed on the same date as another procedure. The documentation must show a separate anatomical site, separate session, or separate clinical indication.
The error: Modifier applied without supporting documentation. Payers audit this heavily, and when documentation doesn’t hold up, services get bundled automatically.
The result: The claim goes out, pays at a bundled rate, and the underpayment never generates a denial you can track.
Revenue risk: Invisible and recurring, until the documentation standard is fixed at the source.
- Modifiers RT & LT – Right Side / Left Side
What changed: The 2026 update shifted how RT and LT interact with multi-level add-on code structures in spinal procedures. The interaction is more complex than it was pre-2026.
The error: Practices that haven’t reviewed bilateral modifier interactions against the 2026 update are running live exposure on every bilateral spine case they bill.
Revenue risk: NCCI edits fire quietly. No denial. Reduced reimbursement that processes cleanly and closes without review.
The Modifiers That Generate the Most Denials in Orthopedic Billing
| Modifier | What It Does | When It's Required | Most Common Error |
|---|---|---|---|
| 51 | Multiple procedures | Secondary and subsequent procedures in same surgical session | Applied to the wrong code; highest-RVU procedure incorrectly takes the reduction |
| 59 | Distinct procedural service | Separate anatomical site, session, or clinical indication on same date | Applied without supporting documentation; payer bundles the service automatically |
| 25 | Significant, separate E/M on procedure day | E/M service above and beyond the procedure itself | Missing documentation showing the visit was medically necessary and separate |
| 57 | Decision for surgery made at E/M visit | E/M visit day before or day of major surgery | Confused with Modifier 25; applied incorrectly to minor procedure encounters |
| XS | Separate structure | More specific version of 59 - different anatomical structure | Underused; practices default to 59 without the specificity payers now require |
| XE | Separate encounter | Distinct session on same date | Rarely used correctly in multi-procedure orthopedic cases |
| RT / LT | Right side / Left side | Bilateral procedure documentation | Incorrect laterality or missing on bilateral spine and joint cases |
| 22 | Increased procedural services | Unusual complexity requiring substantially more time/effort | Vague documentation; applied without explicit narrative in operative note |
How AI-Driven Payer Audits Changed the Rules? And What It’s Costing Orthopedic Practices?
Two years ago, payers were limited by how many human reviewers they could deploy. That limitation is gone.
The Audit Environment Changed. Most Practices Haven’t.
Payers, particularly Medicare Advantage plans, are now running AI-driven claim review tools that cross-reference billing data across years, procedures, and providers at a scale manual review never achieved.
What that means practically:
- A coding error identified today can trigger algorithmic review of every similar claim you submitted in the past 12 to 24 months
- A documentation gap that went undetected in 2024 can surface in a 2026 retrospective audit.
- The exposure is no longer isolated to the individual claim
According to the Office of Inspector General (OIG), these tools are being used to flag discrepancies at scale, and the trend is accelerating through 2026.
Two New Models Adding Friction on Top of That
WISeR Model (2026–2031) Prior authorization is now required for many outpatient orthopedic procedures. Practices with approval rates above 90% earn “gold card” status less paperwork, less friction. Practices below that threshold face increasing delays on every procedure, slowing surgical scheduling and revenue.
Prior Authorization & Interoperability Rules (2026–2027)
Payers are moving to structured, machine-readable clinical data through APIs. Practices still relying on manual chart pulls and unstructured documentation will see authorization turnaround slow significantly, directly impacting OR scheduling and cash flow.
What the Revenue Benchmarks Actually Say
The MGMA benchmark is clear: top-performing specialty practices maintain first-pass clean claim rates at or above 95%, with median days in AR between 32 and 40.
Most orthopedic practices aren’t there.
- Coding and modifier errors alone account for 7%–12% of all claim denials
- Many practices report 10%–15% of claims initially rejected
- A 10% denial rate on a surgical revenue mix means $25,000–$100,000 in delayed or lost collections annually
- Every denied claim that expires past timely filing limits becomes a permanent write-off
Then there’s the rework cost. According to Becker’s Hospital Review, the average cost to rework a single denied claim exceeds $118. For a practice generating 2,000 denials per year, that’s $236,000 spent just to chase revenue the practice had already earned.
The bigger number: most independent orthopedic practices lose 12%–22% of annual revenue to preventable operational gaps. Not clinical ones. Operational ones.
Orthopedic surgery payments have declined 26.2% from 2016 to 2024. Total hip arthroplasty reimbursement is down 39% since 2017. In that environment, revenue leakage from orthopedic coding errors isn’t a back-office nuisance. It’s a margin crisis.
What Is The Financial Impact of Coding Errors on Orthopedic EBITDA?
PE buyers evaluating orthopedic acquisitions in 2025–2026 are applying 7–10x EBITDA multiples to multi-surgeon groups. Every dollar of recovered EBITDA multiplies at that same rate.
The math is straightforward:
A $200,000 annual improvement in net collections, achievable through better modifier accuracy and implant charge capture alone, translates to $1.4M–$2.0M in added enterprise value at a 7–10x multiple.
That’s not a billing number. That’s a valuation outcome.
And for practices not in a near-term transaction, the same math applies to operations. Every $100,000 in preventable denial losses is $100,000 not available for surgeon compensation, equipment investment, or ASC expansion.
Clean billing data, low denial rates, and a high net collection ratio are among the first things a Quality of Earnings analysis examines. Practices that discover coding gaps during PE diligence, instead of before it, face a weaker valuation and a compressed timeline to fix problems that took years to build.
5 Orthopedic Coding Audit Priorities Before Q3 2026
You don’t need to rebuild your revenue cycle. You need to audit the right things, fix what’s broken, and protect what you’ve earned.
1. Audit your top 10 Orthopedic CPT codes against 2026 changes
Not all 418 CPT changes affect your practice equally. Start with your highest-volume codes, joint replacement, spine surgery, shoulder arthroscopy, and verify documentation templates, modifier logic, and add-on code usage are aligned with 2026 definitions.
2. Add a pre-bill quality check on high-value claims
Total joint arthroplasty, multi-level spine fusion, and complex arthroscopy cases should clear a secondary review before submission: CPT code selection, modifier support, documentation completeness, prior authorization status. This prevents the majority of orthopedic claim denials in these categories before they leave the practice.
3. Fix the documentation gap between the OR and the coder
The operative note needs to contain every element such as anatomical location, technique, implant details, laterality, approach, displacement degrees, that allows a coder to bill at the level the procedure actually supports. Updating operative note templates is one of the highest-ROI changes a practice can make.
4. Track global period exposure in both directions
Billing a follow-up visit inside a global period is a compliance risk. Missing billable services genuinely outside it is a revenue leak. Both are common. Both are fixable with the right tracking workflow.
5. Run a revenue-impact simulation by payer
Segment your case mix by procedure and payer type. Estimate the actual impact of the −2.5% efficiency adjustment on your Medicare revenue. Identify which commercial payers mirror that adjustment. Knowing your 2026 exposure, by code, by payer, gives you a baseline to measure against.
How Orthopedic Coding Accuracy Helps Reduce Revenue Leakage
The orthopedic practices that protect their margins in 2026 won’t necessarily be the ones seeing the most patients. They’ll be the ones paying close attention to how they code.
Orthopedic coding accuracy has a direct and measurable impact on collections, cash flow, compliance exposure, and overall revenue cycle health, it’s no longer something that lives quietly in the billing department.
The numbers back this up. According to the Kaufman Hall National Hospital Flash Report, healthcare organizations that tightened their revenue cycle management recovered operating margins of 7% to 12% in 2025. In orthopedics, where reimbursement pressure keeps climbing, even routine coding inconsistencies can quietly drain revenue over time in ways that aren’t immediately obvious.
The environment isn’t getting any easier. CMS reimbursement cuts, tighter CPT 2026 documentation standards, and increasingly sophisticated payer audit systems are putting more pressure on practices to get it right the first time. Modifier errors, documentation gaps, and inconsistent coding patterns don’t just cause one-off denials, they can trigger recurring problems and retrospective audits that are far more disruptive to address after the fact.
The honest reality is that coding errors exist in virtually every practice. The more important question is whether your team catches them first, through proactive internal review, or whether a payer audit catches them for you.
Practices that routinely audit high-risk CPT codes, review modifier usage, evaluate operative note quality, and track denial trends are simply better positioned to protect reimbursement and reduce preventable revenue loss.
Orthopedic Coding FAQs
- 27447 — Total Knee Arthroplasty
- 27130 — Total Hip Arthroplasty
- 29827 — Arthroscopic Rotator Cuff Repair
- 22612 & 22630 — Lumbar Fusion Procedures
- 20610 — Joint Injection Procedures





{kind=link}
{kind=link}