


Table of contents
How Orthopedic Practices Can Prepare For CMS TEAM Model 2026
In July 2025, the Centers for Medicare & Medicaid Services (CMS) launched a game-changing regulation for hospitals and healthcare: the final rule for the Fiscal Year 2026 IPPS and LTCH PPS officially released the TEAM (Transforming Episode Accountability Model) Alternative Payment Model also known as ‘CMS TEAM Model’, and if you’re an orthopedics, this one hits close to home.
Starting January 1, 2026, the hospitals (and their affiliated providers) in selected regions across the United States, should mandatorily adopt TEAM. Yes, unlike the previous bundled payment models like BPCI (which were voluntary), TEAM is mandatory. And it will not just impact hospitals, it will redefine the financial and operational future of caregivers, especially orthopedic practices.
The CMS has clearly outlined in the final rule that the practices will be held accountable for total episode costs, clinical outcomes, and care coordination from surgery through 30 days post-discharge.
What is The CMS TEAM Model?
The TEAM Model is a mandatory, episode-based payment program that holds hospitals responsible for the cost and quality of surgical care, spanning from the procedure through 30 days post-discharge.
The purpose of the TEAM Model
The TEAM Alternative payment is introduced only to restructure payments, but primarily to redefine how surgical care is delivered, tracked, and reimbursed. Through this new payment model, CMS aims to achieve the following:
- Standardized care costs
- Stronger care coordination
- Quality-first reimbursements
Hence, your Orthopedic practice’s performance, from surgical protocols to post-care follow-up, will have a direct influence on how much your hospital partner gets paid (or owes back to CMS).
The Centers for Medicare & Medicaid Services (CMS) recently unveiled the FY 2025 Inpatient Prospective Payment System (IPPS) final regulation, which estimates that TEAM will save the Medicare program approximately $481 million over the 5 performance years (2026 through 2030).
Scope and Timeline:
TEAM will run for five performance years (From January 1, 2026, through December 31, 2030), which covers five major surgical episodes. Under TEAM alternative payment model, acute care hospitals are financially responsible for the full continuum of care i.e, the entire episode of care, which usually starts with surgery and extends to 30 days post-discharge.
For each episode, the CMS calculates a target bundled price, hospitals that deliver care below the threshold while meeting the quality metrics will receive bonus payments, whereas those that transcend the limits will face financial penalties.
This approach gets the orthopedic and surgical teams on the same page to provide smooth, efficient, and top-notch care for their patients.
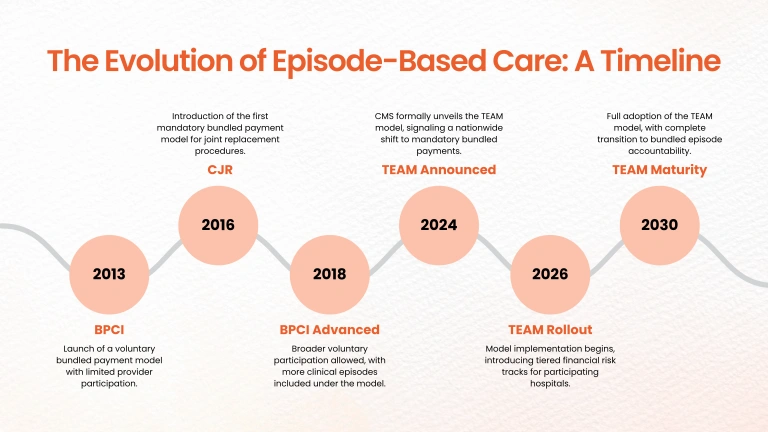
Learning from BPCI: The Foundation for the TEAM Approach
Upon a decade of Medicare payment experimentation, the alternative payment model TEAM is introduced that goes beyond earlier orthopedic-focused bundled programs.
In FY2021, Medicare processed more than 1.1 billion fee-for-service (FFS) claims from over 1.5 million health care providers, making over $424 billion in Medicare payments.
| Previous Model | Key Features | Lessons Applied to TEAM |
|---|---|---|
| BPCI (Bundled Payments for Care Improvement, 2013–2018) | Voluntary model focused on reducing Medicare spending by aligning post-acute care costs across providers.
|
Revealed strong savings potential but variable provider participation and inconsistent quality metrics. |
| CJR (Comprehensive Care for Joint Replacement, 2016–2023) | Mandatory for lower extremity joint replacements in specific areas; introduced standard quality metrics and reconciliation payment structure. |
Demonstrated improved coordination and cost control but limited scalability beyond arthroplasty. |
| BPCI Advanced (2018–2025) | Extended episode duration (up to 90 days post-discharge) and emphasized quality. |
Proven voluntary participation failed to create systemic cost control; informed TEAM’s mandatory structure. |
Navigating the CMS TEAM Model: Key Provisions And Impact
The TEAM model is set to make a significant impact on orthopedic and other specialty surgical practices. And the notable thing about this new payment model is it is mandatory and it directly links the reimbursement and (PROs) patient-reported quality outcomes.
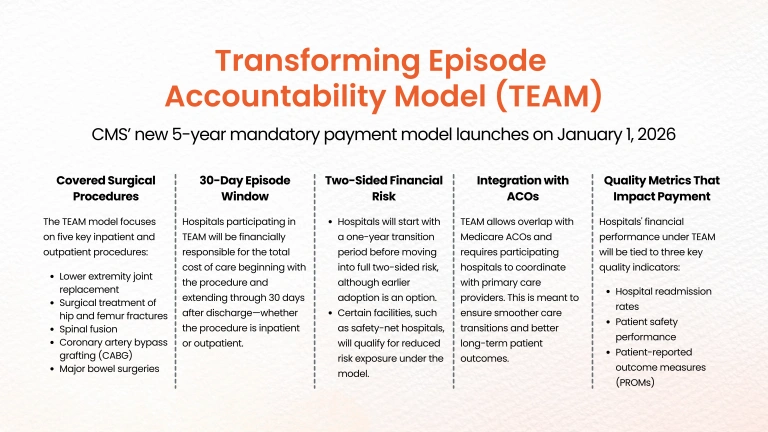
TEAM at a Glance: Covered Areas, Procedures, and Risks
- Applies to hospitals in selected Core-Based Statistical Areas (CBSAs).
- Covers five high-impact surgical categories, including:
- Lower Extremity Joint Replacements (LEJR) (inpatient & outpatient)
- Hip/femur Fracture Treatments
- Spinal Fusions
- Coronary Artery Bypass Graft (CABG)
- Major Bowel Procedures
- Hospitals must manage costs below CMS-set target prices and meet quality benchmarks to earn shared savings.
- Poor performance can result in financial penalties.
While hospitals are directly accountable, orthopedic practices are central to the quality, coordination, and cost-efficiency of each episode, making your performance mission-critical to TEAM outcomes.
Key Objectives of The Alternative Payment Model (TEAM) And What They Mean For Orthopedic Practices
Medicare’s Trustees assume that starting in 2026, clinicians who are not in advanced alternative payment models (A–APMs) will receive lower annual updates to their Medicare physician fee schedule payment rates (0.25 percent per year) than clinicians who are in A–APMs (0.75 percent per year)
| CMS Objective | What It Means for Orthopedic Practices |
|---|---|
Improve care coordination
|
Better alignment with post-acute providers and hospitals is critical, avoiding fragmented handoffs. |
Enhance patient outcomes |
Reduce complications, track PROMs, and engage patients proactively to prevent readmissions. |
Lower Medicare spending |
Avoid overuse of costly post-op care and standardize pathways. |
Promote primary care continuity |
Ensure timely post-discharge referrals to PCPs or ACOs, CMS is watching closely. |
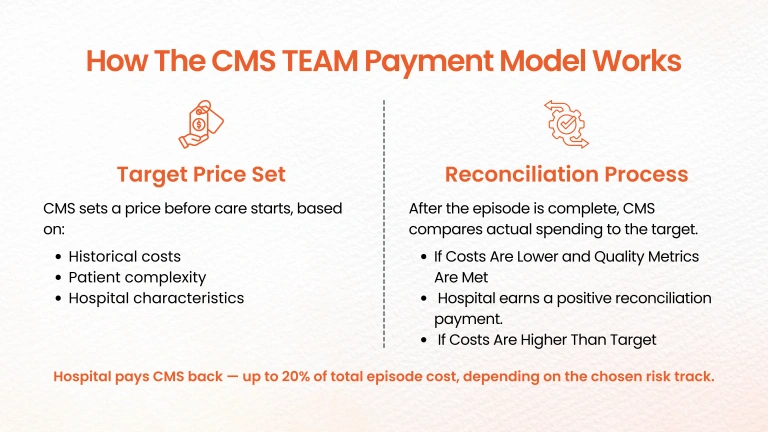
The CMS TEAM Model Financial Structure: What’s at Stake
Hospitals are reimbursed through a retrospective reconciliation process. Here’s how it works:
- CMS sets target prices in advance for each episode, based on historical costs, adjusted for patient complexity and hospital characteristics.
- After care is delivered, CMS compares actual episode spending to the target.
- If costs are lower and quality metrics are met, the hospital earns a positive reconciliation payment.
- If costs exceed the target, the hospital owes money back to CMS, up to 20% of the total episode cost, depending on risk track.
While hospitals bear this financial risk directly, orthopedic teams influence every cost driver: surgical supply use, OR time, post-acute care referrals, readmissions, and complications.
TEAM Participation Tracks & Risk Levels
CMS offers three levels of financial risk through “tracks”:
- Track 1: Upside-only (no penalties), capped gains. Available for all hospitals in year 1; extended through year 3 for safety-net facilities.
- Track 2: Moderate risk and reward (5% gain/loss cap). For rural, sole community, and essential access hospitals.
- Track 3: Full-risk model (20% gain/loss cap). Available to all participants throughout the model.
This structure gives hospitals time to adapt, but orthopedic partners must also scale up readiness in parallel.
The Strategic Impact of TEAM on Orthopedic Episode Care
Even though hospitals are the primary participants, the CMS TEAM Model reshapes the environment orthopedic surgeons operate in. Your clinical decisions, discharge plans, and care coordination all affect episode costs, readmissions, and patient outcomes.
Here’s how TEAM impacts your practice:
Mandatory Participation in Many Regions
Unlike previous bundled payment models like BPCI, TEAM does not allow hospitals in selected regions to opt out. This means orthopedic groups must be prepared to participate, whether they feel ready or not.
High-Stakes Reimbursement Tied to Performance
CMS sets target episode prices that include built-in savings assumptions. To succeed, hospitals and providers must deliver care more efficiently than historical benchmarks, while maintaining or improving quality.
Stricter Quality & Outcome Requirements
Hospitals must meet specific clinical and patient-reported outcome measures (PROMs) to qualify for shared savings. If your practice isn’t already tracking outcomes consistently, you may be the weak link in the chain.
So, it is crucial for orthopedic providers to strongly focus on collecting meaningful data than ever before. This also helps you to consistently deliver high-quality, and outcome-driven care to stay competitive and financially viable.
Why TEAM Poses New Financial Challenges for Orthopedic Practices
Mandatory Participation That Increases Accountability
Unlike previous models, orthopedic practices operating in TEAM-selected regions cannot opt out. This makes active participation and strategic alignment with hospital partners non-negotiable for financial survival.
Aggressive Target Pricing Demands Cost Control
CMS sets target prices with built-in discounts, expecting providers to cut costs below historical averages to avoid penalties. For orthopedic episodes—which typically involve high post-acute care variability, this requires precise control of care pathways and associated costs.
Quality and Outcomes Drive Payment Adjustments
Under TEAM, quality reporting is not optional. Failure to meet performance benchmarks or to consistently collect and report Patient-Reported Outcome Measures (PROMs) can directly reduce potential incentive payments, no matter how much cost savings are achieved.
The TEAM Effect: What’s Changing for Orthopedic Providers
Though TEAM accountability primarily falls on participating hospitals, orthopedic practices and surgeons play a direct and essential role in the model’s outcomes.
Orthopedic procedures, particularly joint replacements, hip/femur fracture repair, and spinal fusion, constitute some of Medicare’s most common and cost-intensive episodes, making orthopedic teams crucial to success within TEAM.
Here’s how it impacts your practice:
Surgical Outcomes Drive Hospital Revenues
Team payments to hospitals are based on their Composite Quality Score (CQS), which includes orthopedic-specific measures like patient-reported outcome measures (PROMs), readmission, and discharge efficiency.
Your surgical outcomes, recovery process, and rehab coordination now directly tie to bottom-line performance.
Data and Reporting Requirements Increase
Hospitals and orthopedic staff must gather and report outcomes data, including patient-reported outcomes, a new measure in addition to clinical measures.
Orthopedic surgeons and administrators will need to enhance documentation systems and institute RCM systems capable of accommodating new reporting requirements.
New Opportunities for Financial Partnerships
Although orthopedic physician groups are not immediately in convening model status, TEAM can get hospitals to pledge co-management or gainsharing arrangements and compensate orthopedic providers engaged in cost and quality targets.
Practice groups that manage perioperative care more logically, lower readmissions, and optimize coordination can share profit.
Post-Acute Cost Control and Discharge Planning Are Most Important
Medicare statistics have revealed that orthopedic post-acute care (rehab, home health, and skilled nursing) are most likely to be the source of highest cost variation.
This new alternative payment model TEAM promotes good discharge and recovery processes without compromising the outcomes. It is a great opportunity for your practice to show leadership and alignment with hospital efforts.
Integration with Digital and Remote Care
TEAM’s introduction aligns with CMS’s vision of virtual care and remote patient monitoring (RPM) in 2026.
Orthopedic practices embracing digital follow-up care and remote therapy modalities can reduce readmissions, improve outcomes, and improve value positioning in the model.
Episode Cost Calculations Under the CMS TEAM Model: What’s Counted and What’s Not
Under Medicare’s TEAM (Transforming Episode Accountability Model), an ‘episode’ includes a patient’s surgical hospitalization and all related care within 30 days after discharge.
CMS looks at the entire recovery journey, not just what happens in the OR.
What’s Included in the Episode Cost Calculation Under TEAM Model
Each TEAM episode combines the total Medicare-covered costs from the index surgery and all medically related services post-discharge. Here’s what counts:
- Hospital stay (DRG payment) – Medicare’s bundled payment for the inpatient surgery.
- Readmissions – Any unplanned hospital stays within 30 days.
- Physician and practitioner services (Part B) – Such as the surgeon, consultants, anesthesiologist, and all post-op follow-ups.
- Post-acute care (PAC) – Skilled nursing facility (SNF), inpatient rehab (IRF), home health (HHA), or long-term care hospital (LTCH) services.
- Outpatient services – Services include imaging, physical therapy, labs, and emergency visits.
- Durable medical equipment (DME) – Including braces, walkers, or mobility aids.
- Hospice – If initiated within 30 days of discharge.
Not included:
Unrelated elective surgeries or Medicare Part D prescription drug costs.
Example: A Typical TEAM Episode for Lumbar Spinal Fusion
Let’s look at how a common orthopedic procedure, lumbar spinal fusion might add up under the CMS TEAM model.
| Category | Estimated Medicare Cost |
|---|---|
Hospital DRG payment
|
$18,000 |
Surgeon and physician fees |
$5,000 |
Anesthesia |
$1,300 |
SNF stay (5–7 days) |
$5,800 |
Home health visits |
$1,200 |
Outpatient physical therapy |
$1,500 |
DME (brace, walker, etc.) |
$600 |
Readmissions or ED visits |
$2,200 |
Other outpatient labs/imaging |
$900 |
Total Episode Cost |
$36,500 |
Now, if CMS sets your region’s target price at $35,000, you’re $1,500 over target—which could result in a repayment penalty.
How Medicare Establishes Episode Target Prices Under TEAM
Medicare bases episode target prices on regional spending history, typically the past three years of claims data.
They then apply a discount (around 1.5–3%) to ensure overall savings for Medicare.
Example:
- Regional average spending: $36,000
- CMS discount: 3%
- Target price: $34,920
Hospitals must perform below this threshold to earn reconciliation bonuses.
Reconciliation: Bonuses and Penalties
Every six months, CMS compares your actual spending against your cumulative target price:
- If you spend less than the target: you earn a bonus.
- If you spend more than the target: you owe Medicare the difference.
Example:
- 150 spinal fusion episodes
- Target price: $35,000
- Actual cost per episode: $36,500
$1,500 × 150 = $225,000 penalty owed to CMS
If you bring costs down to $34,000 per episode, you save $150,000 total — and earn that as a bonus.
Risk Caps: Protecting Hospitals from Major Losses
CMS caps potential gains and losses to balance accountability and protect hospitals:
| Track | Risk Type | Financial Exposure |
|---|---|---|
| Track 1 | Upside only
|
Earn bonuses only, no penalties |
| Track 2 & 3 | Two-sided
|
Bonuses and penalties (usually capped at 20% of total episode payments) |
So, if your hospital receives $5 million in annual TEAM payments, your max risk (or bonus) would be $1 million under a 20% cap.
How Quality Affects Payment Outcomes
TEAM isn’t just about cost control, quality performance matters too.
Your reconciliation payment is adjusted based on metrics such as:
- 30-day readmission rates
- Complication and infection rates
- Patient-reported outcomes (PROMs)
- Patient experience (HCAHPS)
High performance = higher bonus
Low performance = reduced bonus or added penalty
Typical quality adjustments range around ±3% of your total reconciliation amount.
Volume Weighting: Giving Weight Where It Matters
CMS gives more weight to procedures you perform more often.
If your hospital does:
- 200 spinal fusions
- 50 shoulder replacements
Spine outcomes account for 80% of your quality score.
This ensures your largest service lines influence your final score proportionately.
Quality Adjustment in Action
Let’s revisit our earlier example:
- 150 spinal fusion episodes
- Target: $35,000 → Total $5.25M
- Actual: $34,000 → $150,000 under target
- Quality bonus: +2%
Additional +2% of $5.25M = $105,000 bonus
Total reconciliation = $150,000 + $105,000 = $255,000 reward
If quality were -2%, you’d lose $105,000 and reduce your savings to $45,000.
Preparing Your Orthopedic Practice to Succeed Under TEAM
- Prevent avoidable readmissions and complications
Adopt typical pathways to prevent infection, support early mobilization and multimodal pain control. When you avoid readmissions, you can save reasonable costs. - Optimize discharge destinations
Advise home discharge when necessary, home health is less expensive than SNF. - Collaborate with efficient post-acute partners
Build connections with SNFs and home health agencies that foster shorter stays and better outcomes. - Eliminate unnecessary utilization
Minimize your ED visits by avoiding multiple consults, limiting unneeded imaging, and doing robust post-discharge follow-up.
Internal vs. External Cost Control
- Internal savings includes negotiating implant prices, improving OR efficiency etc, which helps to increase hospital margins under fixed DRG payments.
- External savings from fewer readmissions, shorter SNF stays will help you lower Medicare’s total spend, and directly improve your reconciliation performance.
To align your practice under TEAM and orthopedic revenue cycle management goals, orthopedic programs need to balance clinical excellence, efficient usage of resources, and proactive care coordination.
How RCM Solutions Help Orthopedic Practices Scale Under TEAM
1. Unify Clinical and Financial Data for Real-Time Decision-Making
RCM solutions that integrate clinical documentation, quality metrics, and billing data help orthopedic providers to manage the entire patient episode, before, during, and after surgery. This gives your real-time visibility into the orthopedic practice performance and allows you to identify risks at the early stage and perform timely interventions.
2. Automate Compliance and Quality Reporting
One of the effective ways to reduce administrative burden and ensure compliance with TEAM’s quality standards is to streamline PROMs collection and reporting. BillingParadise offers automated RCM workflow to help you with accurate and timely claim submissions, and strengthen your billing foundation.
Medicare’s Trustees assume that starting in 2026, clinicians who are not in advanced alternative payment models (A–APMs) will receive lower annual updates to their Medicare physician fee schedule payment rates (0.25 percent per year) than clinicians who are in A–APMs (0.75 percent per year)
3. Improve Coding Accuracy and Denial Management
This episode-based billing under the TEAM model comes with certain complexities. In order to deal with that, you need precise, procedure-specific billing expertise such as certified medical coders and technology-enabled RCM services providers.
By outsourcing to a orthopedic billing partner, you will substantially prevent coding errors, increase first-pass claim acceptance rates, and master denial management to recover lost revenue quickly.
4. Optimize Post-Acute Care Collaboration
Coordination across care settings is critical to controlling costs and minimizing readmissions. The automated RCM systems will track referrals, discharge plans, and utilization of followup-care, which help your orthopedic practice to remain aligned with care plans that support cost-efficiency and quality care goals.
5. Enable Predictive Performance Monitoring
Predictive analytics tools within RCM platforms identify financial and clinical risks before they impact reimbursement. This enables orthopedic practices to proactively adjust workflows, optimize resource use, and continuously improve their performance under TEAM.
As an RCM solutions provider, we understand the operational complexity and financial pressure this model imposes, and how advanced revenue cycle management strategies can turn risk into opportunity.
How BillingParadise Helps You Empower Your Orthopedic Practice in the TEAM Era
The transition to the CMS Transforming Episode Accountability Model (TEAM) marks a pivotal shift for orthopedic practices, from retrospective reconciliation to prospective episode-based TEAM Alternative payments tied to quality, efficiency, and equity.
We help your practice not just adapt, but lead, in this new value-driven framework.
Unify Clinical, Financial, and Quality Insights
Integrated dashboards bring together cost data, quality metrics, and patient-reported outcome measures (PROMs) across every orthopedic episode.
Gain real-time visibility into episode cost drivers, risk-adjusted benchmarks, and quality performance to stay ahead of CMS target thresholds.
Streamline TEAM Compliance & Quality Reporting
The TEAM model links payment to quality and health equity metrics. At BillingParadise, we help you automate PROMs capture, documentation, and submission, directly within your EHR or billing system, reducing manual effort and ensuring accurate, timely reporting for each episode of care.
Optimize Episode Performance & Denial Prevention
TEAM participation increases financial risk exposure tied to episode cost and quality outliers.
Our AI-powered denial management solution identifies coding errors, improper episode attribution, and documentation gaps before claims submission, safeguarding revenue integrity and minimizing post-episode penalties.
Enable Strategic Forecasting & Reconciliation Readiness
We model episode-level cost projections and target price variances, helping orthopedic groups forecast financial outcomes under TEAM’s risk-adjusted payment methodology.
This enables proactive decisions, from care coordination to cost containment, before CMS reconciliation.
Align Operations Across the Care Continuum
TEAM emphasizes collaboration across hospitals, post-acute providers, and specialists.
We help you bridge operational silos, ensuring seamless episode coordination, shared data visibility, and documentation alignment across every partner involved in the orthopedic care pathway.
With our RCM solutions, orthopedic practices gain the operational intelligence and automation needed to succeed in a prospective, performance-based payment world.
We help you lead with data, strengthen compliance, and drive financial success — not just participate in the TEAM transition.
From Volume to Value: Align, Adapt & Advance Your Orthopedic Care Under TEAM Model
The CMS TEAM Model represents a watershed shift in how orthopedic episodes are reimbursed and managed, mandating deeper integration, accountability, and data-driven care.
Orthopedic practices that proactively adapt operational, clinical, and financial systems will thrive under TEAM, enhancing both patient outcomes and practice sustainability.
Starting now, orthopedic practice leaders must engage their hospital partners, optimize revenue cycle workflows, embrace quality measurement, improve care coordination, and build financial agility.
With the right strategies, the TEAM Model can transform orthopedic care delivery into a more efficient, patient-centered, and financially rewarding enterprise.





{kind=link}
{kind=link}
{kind=link}