

Table of contents
Key Takeaways:
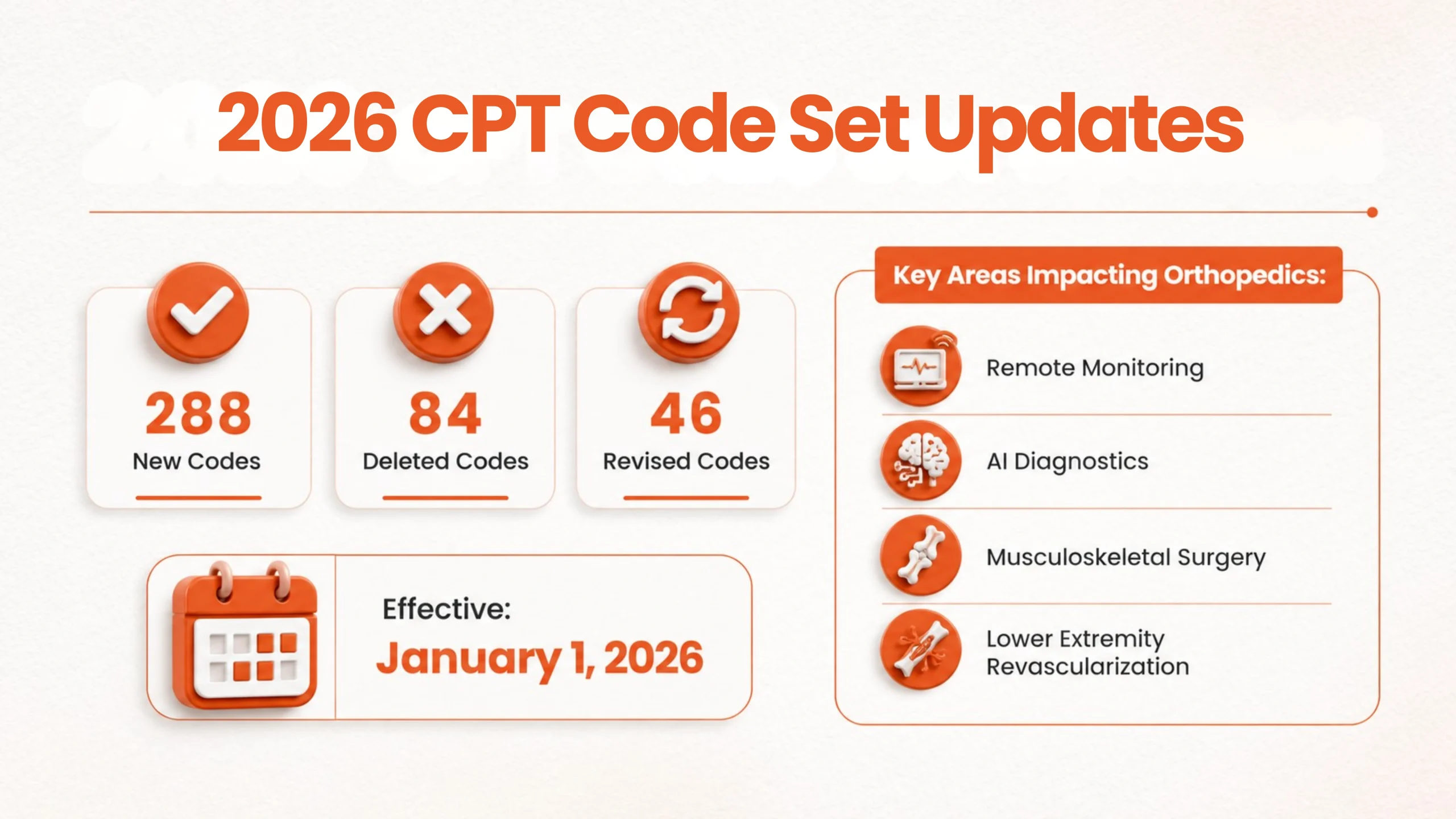
- The AMA CPT 2026 code set has rolled out 418 changes, 288 new codes, 84 deletions, and 46 revisions, starting January 1, 2026.
- The CPT update directly impacts orthopedic billing in four key areas: remote monitoring, AI diagnostics, musculoskeletal surgical codes, and lower extremity revascularization.
- If you’re billing with outdated or deleted CPT codes, expect your claims to be denied every time, and those denials are completely avoidable.
What Do the 2026 CPT Code Set Changes Mean for Orthopedics?
If your practice is experiencing more claim denials before, even though your clinician’s doing the same procedures, following the same workflow, and your patient volumes look steady.
And honestly, those monthly denial reports keep showing issues that don’t match what you see day-to-day.
The real problem isn’t always inside your practice. Orthopedic coding rules change, payers update their policies, and documentation requirements get tougher. That drives up denials, even when everything on your side seems smooth.
That‘s why 2026 CPT code updates matter for orthopedic revenue cycle management.
How outdated coding could cost an orthopedic practice?
Outdated orthopedic coding will not only slow down your reimbursements, but also cause revenue leakage with nearly every claim you submit.
If your orthopedic practice bills more than 50 procedures a month, the 2026 CPT coding changes will impact a significant amount of your reimbursement workflow. Effective January 1, 2026, the American Medical Association has introduced a new CPT code set while deleting and revising others, which created an impact in medical coding accuracy, claim submission and revenue capture.
For orthopedic providers, the impact is very high as they deal with complex procedures, extensive documentation and tightening financial margins which demands absolute precision in medical coding.
The average coding-related claim denial dollar amount rose 126% in 2024, from $297 to $631 per denial.
If you’re an orthopedic CFO or revenue cycle leader overseeing orthopedic billing operations, understanding the 2026 CPT coding changes is essential to ensure smooth reimbursement and protect your revenue.
What Orthopedic Practices Should Know About The 2026 CPT Coding Changes?
The AMA has rolled out the CPT 2026 code set, and there’s a lot to uncover. This includes:
- 288 new CPT codes
- 84 deleted codes
- 46 revised code descriptions
2026 CPT Coding Updates for Orthopedics
| Change Type | Count | Notable Areas Affected |
| New codes | 288 | RPM/RTM, AI diagnostics, musculoskeletal surgery, revascularization |
| Deleted codes | 84 | Outdated remote monitoring, legacy surgical descriptors |
| Revised code descriptions | 46 | Joint arthrodesis, sacroiliac fusion, hardware placement |
| Total changes | 418 | Across all specialties |
For orthopedic billing, specifically, the coding changes that carry the most financial weight fall into four areas:
- Remote monitoring
- AI diagnostic coding
- Musculoskeletal surgical codes
- Lower extremity revascularization
As part of 418 editorial changes in the CPT code set, 288 new CPT codes are implemented. These codes have implications on various areas: from digital health and AI tools to sharper surgical and diagnostic coding.
If your orthopedic practice offers remote monitoring, or specialized procedures, make sure your billing team uses the new codes. The new codes especially matter for the way you report surgeries, track patients after procedures, and bill for the latest care options.
“The standardization of CPT codes has greatly streamlined billing, coding, and reimbursement – however, at the same time, it has harmed the same process by not allowing for grading of complexity.” Said Dr. Richard Yoon, MD, Director of Orthopedic Research and Division of Orthopedic Trauma and Adult Reconstruction Surgery at Jersey City Medical Center



Key Areas That Are Impacted By CPT Updates in Orthopedic Billing
1. How did the 2026 CPT updates change remote monitoring billing?
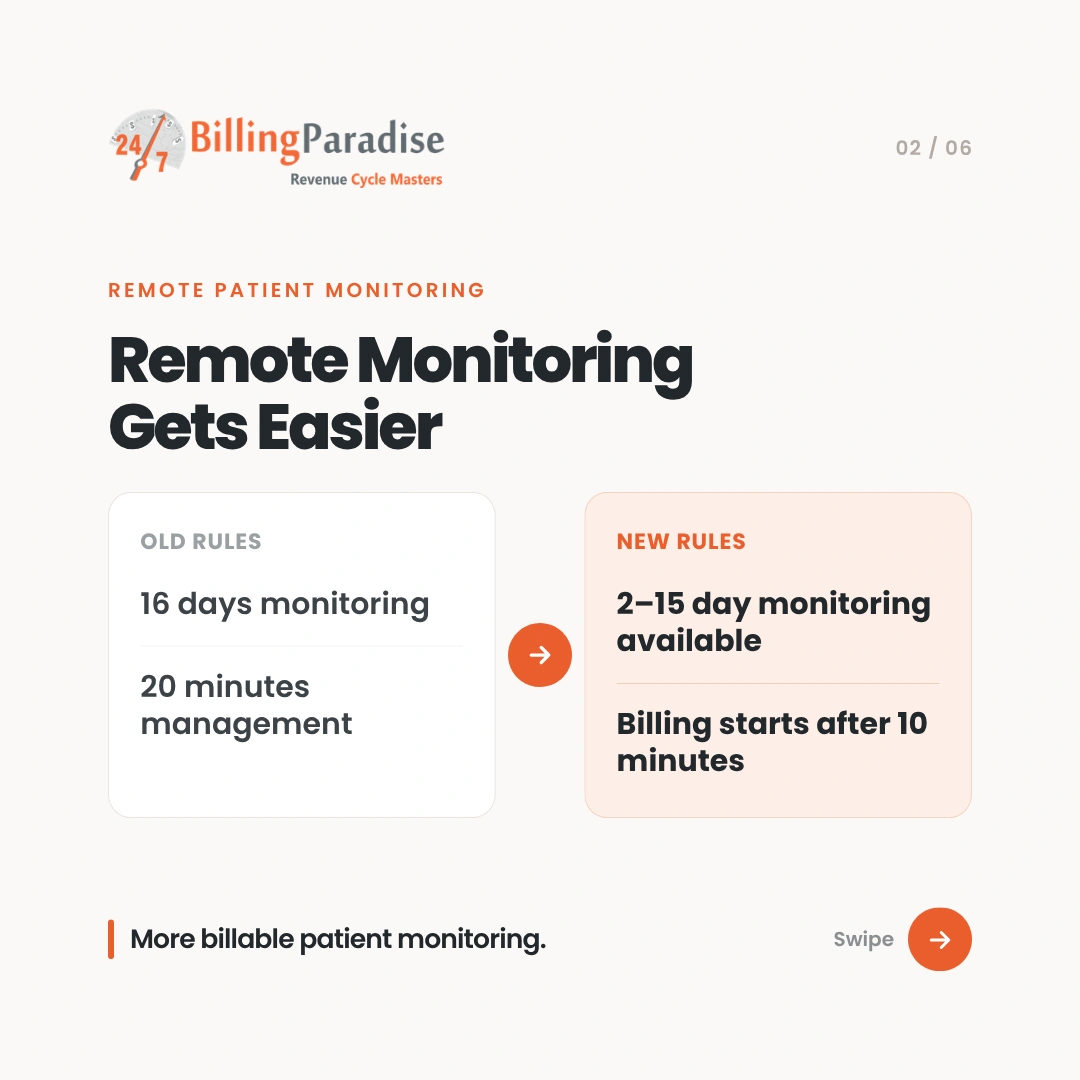
Before, all remote monitoring codes held the providers’ hands; practices needed at least 16 days per month of data before they could be paid. And 20+ minutes of interaction before they could bill for treatment management-many scenarios where some remote monitoring still served an important purpose fell outside those categories as unbillable.
The CPT update for 2026 corrects this. Providers no longer need at least 16 days of continuous data or 20+ minutes of intervention time before they are able to bill for remote monitoring. This means greater latitude for practices as they take on more complex remote care and gain opportunities for previously non-reimbursed activities to be billed.
For instance, an orthopedic practice could now remotely monitor recovery from surgery or chronic joint pain for between 7 and 10 days and still be reimbursed at code 99XX4 and 98XX5. This was previously unheard of.
Some of the old RPM codes still exist, but the medical billing rules just got updated:
99445 – RPM: device supply and recordings (now covers 2 to 15 days)
99454 – RPM device supply (now 16 to 30 days)
99470 – RPM treatment management (first 10 minutes)
99457 – RPM treatment management (first 20 minutes)
99458 – RPM treatment management (each extra 20 minutes)
Now, you can start billing after just 10 minutes. This lines up way better with how clinicians actually work.
New RPM/RTM CPT Codes & Medicare Reimbursement
| CPT Code | Description | 2026 Medicare Reimbursement |
| 99445 (new) | RPM device supply, 2–15 days of data | $47/month |
| 99454 (revised) | RPM device supply, 16–30 days of data | $52.11/month |
| 99470 (new) | RPM treatment management, first 10–19 min | $26.05/month |
| 99457 (revised) | RPM treatment management, first 20 min | $51.77/month |
| 99458 | RPM treatment management, each add’l 20 min | $41/month |
| 98XX5 (new) | RTM – musculoskeletal system, 2–15 days | Pending payer schedules |
| 98XX7 (new) | RTM treatment management, first 10–19 min | Pending payer schedules |
The American Association of Hip and Knee Surgeons (AAHKS) reported that the 2025 Medicare Physician Fee Schedule Final Rule’s 2.9% conversion factor reduction translated to roughly a 1% overall decline in Medicare reimbursements to orthopedic surgeons, with total knee arthroplasty (CPT 27447) reimbursement falling from $1,262.68 in 2024 to $1,257.68 in 2025.
Is your medical coding process equipped to handle the reimbursement challenges ahead? Get a clear answer with our concise coding audit report.
2. What are the new AI diagnostic codes, and should orthopedic practices bill them?
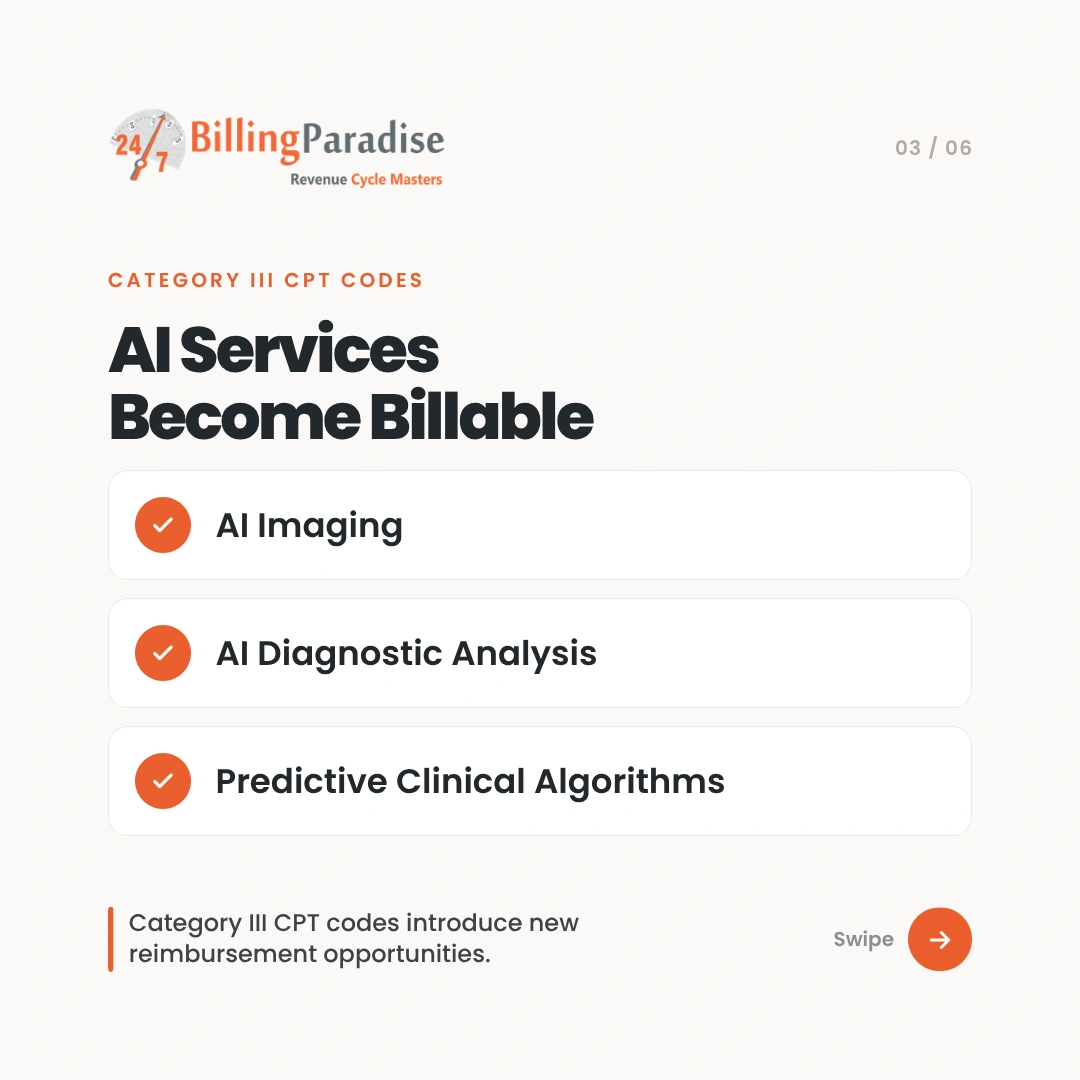
The AMA is adding new Category III CPT codes (Augmented Intelligence Codes ) to describe AI-powered diagnostic and analytic services. This means various types of machine-assisted clinical work are now billable.
Examples include:
- AI assessment of coronary atherosclerotic plaque
- Perivascular fat analysis for cardiac risk
- Multi-spectral imaging of burn wounds
- Detection of cardiac dysfunction by an AI algorithm
Remember these Category III codes are still emerging tech and many payers will need additional verification prior to covering them.
3. What surgical CPT codes changed for orthopedic procedures?
Although the 2026 CPT code set is not solely for orthopedics, many surgical codes directly impact musculoskeletal care:
For Example:
CPT 27713 Osteotomy of the tibia with an externally controlled intramedullary lengthening device, including imaging, alignment, and device management, recognizing technological advancements in limb lengthening and deformity correction.
Orthopedics practices should begin to bill this code for limb lengthening and deformity correction.
Changes in procedures, such as arthrodesis of joints and hardware application, especially Sacroiliac fusion, will also be observed with adjusted wording rather than all brand new codes.
4. How does the lower extremity revascularization rebuild affect orthopedic billing?
These vascular codes are not solely for vascular surgery but will impact orthopedic practitioners caring for limb ischemia.
46 new codes now replace the previous group of lower extremity revascularization codes for both ambulatory and complex surgical approaches in greater detail.
Thus, coding and clinical staff should immediately implement training.
Failure to do so can nearly guarantee denied endovascular and/or bypass claim forms.
Why Do These Coding Updates Really Matter for Orthopedic Billing?
- New RPM/RTM codes bring in the revenue that has been leaking: In many cases, practices can now bill for remote or short-term monitoring services that previously went unpaid.Lower time thresholds allow you to get reimbursed for work that you’re already doing. This means that the lost revenue through non-reimbursed telehealth is reduced.
- AI augmentation codes allow you to be properly reimbursed: If your practice utilizes AI for diagnostic imaging or other clinical analysis, this new set of codes means you are finally able to capture value in your clinical practice for services you previously had no means to bill for.
- More precise procedure codes mean less denied claims: For example, when you use 27713 instead of a less specific code, your claims and clinical documentation are better aligned. The payer is less likely to push back, and your acceptance rate will increase.
How Many CPT Codes Change Every Year, And Why Does The Pace Matter For Orthopedic Billing?
Each year, the CPT codes are updated by the American Medical Association on January 1. As the volume of changes to the codes has been steadily increasing.
In January 2023, there were 225 newly created codes, 75 codes deleted, and 93 codes that were changed for a total of 393 editorial changes.
For 2025 there were 270 new codes, 112 deleted codes, and 38 changed codes for a total of 420 edits. For 2026 the total number of changes was 418, including 288 newly created codes.
| Code Year | New Codes | Deleted Codes | Revised Codes | Total Changes |
| 2023 | 225 | 75 | 93 | 393 |
| 2025 | 270 | 112 | 38 | 420 |
| 2026 | 288 | 84 | 46 | 418 |
Why Do Coding Errors Take Months to Surface in Orthopedic Revenue Cycles?
For the majority of specialties, the annual refresh falls under the area of responsibility for the billing department. In the case of orthopedics, however, the inherent risks associated with the annual cycle are disproportionately higher than most specialties.
Because orthopaedics includes high dollar per claim amounts, highly complex modifier logic, stringent documentation requirements related to implants, and substantial scrutiny by payers.
Therefore, a coding error that costs a primary care practitioner $80 will cost the orthopaedic practitioner $600 (or more).
Each year, orthopaedic facilities are forced to operate under similar constraints as they enter January.
The first of the year is the effective date of the new CPT codes, payers have updated their fee schedules, and any billing templates or charge master systems that were not updated prior to year-end will now generate claims that are either denied or will be reimbursed at the incorrect rate.
Whereas the annual orthopedic coding update for most specialties is generally a rather minor administrative task, for orthopaedics it is one of the most critical events in the revenue cycle.
Because high procedure dollar amounts, complex modifier requirements, and rules individual payer rules creates an environment where any errors occurring in the coding process at the start of the year could take the entire CY to get through the collections process before the error is identified.
It is this compounding effect that many of the CFOs for orthopedic facilities regularly overlook. An error occurring in January does not create a January denial.
Rather, it ultimately results in an accounts receivable (AR) issue in Q2, an audit flag (due to overpayment) in Q3, and the introduction of a write-off discussion in Q4.
How Can Orthopedic CFOs Quantify The Revenue Risk From CPT Code Transitions?
Most orthopedic CFOs identify revenue losses due to CPT transitions only after it’s happened, usually seeing them in a denial report that shows an unexpected rise. This leads to cash flow issues, delays in coding work, and ARs that are far worse than anticipated.
With the new CPT coding rules set to go live with 288 new codes and a total of 418 changes, simply managing reactively is not feasible for a 10-25 provider orthopedic practice. The risks are too broad, the volume is too high, and payers have too little tolerance for delay.
To outpace reactive orthopedic providers in 2026, CFOs need one key skill: predicting the impact of CPT-driven revenue risk before any claim is even submitted. It is important to include Medical Coding audits on the CFO roadmap.
Let us break down the process of converting uncertainty surrounding the CPT changes into financial projections that a CFO can take action on.
The Revenue Risk Model: The Four Stages to Quantify Exposure
Stage 1: How do you identify which CPT changes actually affect your practice?
The first step involves categorization, but of your practice’s current billing mix, not the entire set of new codes. Your top 50-100 CPT codes from 2025 based on claim volume and net revenue should be assessed according to a three-category risk level:
| Risk Category | Code Type | Financial Exposure Profile |
| High Uncertainty | New codes (288) | Unknown payer adjudication; LCD gaps may cause broad first-pass rejection in Q1 |
| Moderate Risk | Revised codes (~60) | Mismatches between 2025 coding documentation templates and 2026 code language, along with new bundling rules |
| High Denial Risk | Deleted codes (70+) | Any claim submitted with a deleted code is a 100% preventable denial and should result in automatic rejection |
This stage will not produce a list of every CPT code ever written, but rather a prioritized risk registry for your practice’s typical billing codes.
Typically, 15-30 codes at most account for the bulk of the financial risk in a 10-25 physician orthopedic group.
Where this data comes from: Combine the AMA CPT 2026 document with the top codes from your practice management system for 2025. With collaboration between your RCM team or billing partner, you can get this crosswalk within 2-3 business days.
Stage 2: Which procedures carry the most concentrated revenue exposure?
With a risk-stratified list of codes, your next focus is the amount of revenue that hinges on each risk category. This step examines the relationship between the procedures you perform and the revenue generated.
The aim is to identify the specific CPT changes that are likely to have the largest impact. In a 15-provider orthopedic group, for example, the top 20 revenue-producing CPT codes often comprise 65-75% of overall annual revenue.
This is a concentrated exposure point but can also be an efficiency benefit, allowing you to protect the vast majority of your revenue by addressing a small number of codes properly.
The analysis should answer the following three questions:
1. How do high-frequency codes fall into revised or deleted categories?
A code used 1,200 times a year at an average reimbursement of $1,800 represents $2.16 million in annual revenue. A 3% rise in denials for this one code translates to $64,800 in lost revenue.
2. Are new 2026 codes replacing 2025 codes in your standard billing workflow?
If a new 2026 code replaces a 2025 code your practice billed 800 times last year, correct coding for the new code must begin on January 1st or the claim will go to manual review or be denied entirely.
3. Which subspecialty areas are the most vulnerable to concentrated exposure?
Generally, joint replacement, spine, and sports medicine have the highest individual claim reimbursement rates in orthopedics. A volume sensitivity analysis will help confirm whether your exposure is contained within one specialty or is more widespread.
Data from MGMA’s Physician Compensation and Production Survey shows that orthopedic groups in the top quartile of revenue performance bill 85% or more of net collections from their top 25 codes. This concentration validates volume sensitivity analysis.
Stage 3: What does the revenue leakage actually look like in dollar terms?
This step transforms vague risk into specific dollar amounts for your CFO’s quarterly plan. Using your volume-weighted, risk-stratified list, apply error rate assumptions for each risk category:
Denials by Risk Category
| Error Rate Scenario | New Codes | Revised Codes | Deleted Codes |
| Conservative (Well-prepared) | 1–2% | 2–3% | 0% (Fully-Suppressed) |
| Moderate (average transition) | 3–5% | 4–6% | 0.5% (Partial Suppression) |
| Stress (unprepared) | 6–10% | 7–10% | 2–3% (Significant Exposure) |
Denial probabilities should also reflect payer specifics. AI claims editing often processes new NCCI edits more quickly than Medicare MACs with their formal implementation process. Your top 3 commercial payers should each have their own specific denial probability estimate.
Applying this to an example practice: An $18 million annual net revenue, 15-physician orthopedic group collects 70% of revenue ($12.6 million) from its top 20 codes. Eight of these codes fall into revised or new categories in 2026, representing $7.2 million in exposed revenue.
A moderate 3% blended denial rate results in an annual revenue leakage of $216,000, concentrated in Q1 2026, the period when transition errors typically peak.
Under a stress scenario with a 6% denial rate, this number increases to $432,000, a critical figure for an orthopedic CFO’s risk register.
CFO Insight: The simulated losses aren’t typically permanent. Most denials can be appealed. These are the cash flow disruptions and administrative burdens associated with chasing those denials. A $432,000 denial volume can cost $40,000-$80,000 in administrative expenses to recover, even with high appeal success rates.
Stage 4: How do CPT transitions affect cash flow beyond direct denials?
In addition to direct denials, CFOs consistently overlook the secondary, and often more substantial, impact of CPT transitions: accounts receivable extension. Claims may eventually be paid correctly, but may take an additional 7-21 days to get paid due to manual review, increased documentation needs, or payer processing lags as new code logic is incorporated.
This delay has a tangible impact on cash flow, and often won’t appear on revenue reports, but will be evident in cash flow statements and bank account balances, when the CFO has already made commitments to Q1 operating expenses.
Your AR delay model should include:
Average daily revenue: Annual net collections % 365
Additional AR Days: Average daily revenue x estimated number of additional AR days x percentage of claims impacted
For the $18 million practice example, with $49,315 average daily revenue, and an estimated 15% of claims experiencing a 14-day delay:
14 days × $49,315 × 15% = $103,562 in cash flow displacement in a quarter
Anticipating this figure allows a CFO to better plan Quarterly credit line needs, cash reserves, and expense timing.
How To Prepare Your Orthopedic Practice For 2026 CPT Coding Changes?
- Update your code references now
Train coders on the 2026 CPT set and the entire updated code set is available at ama-assn.org. Start by focusing on what has been deleted.
- Overhaul operative note templates
Match documentation with what the codes require, especially in cases of CPT 27713, changes in sacroiliac fusion, and joint arthrodesis descriptors; Without sufficient notes, coders are unable to correctly code your work.
- Test your new codes prior to live use
Submit test claims with new codes to major payers to iron out rejection issues in a low-stakes environment before they begin to impact your revenue.
- Conduct Coding Audits Every Quarter
Errors concentrate during the first three months of a new code set’s implementation. It is far cheaper to catch coding errors early than to deal with their impact later. - Review RPM/RTM workflows
If your practice provides any kind of remote monitoring, document your process and review it against the new code thresholds. The two coding changes most likely to impact your revenue directly will be the requirement to monitor for at least 10 minutes at a time, and the mandate to review no more than two to 15 days.
Real Orthopedic Revenue Risk Isn’t CPT Change, It’s Financial Blindspot – Fix Them Today!
The biggest threat in 2026 is not learning the new codes; it is billing with the old way of thinking.
The 2026 CPT updates represent more than mere coding changes; they mean revenue changes for orthopedic practices. New remote monitoring options to modified surgical codes-being aware of the changes is key to avoiding denials and maximizing reimbursement, and maintaining compliance.
Practices that plan ahead by updating their documentation and training their coding teams will be the ones that are most successful in optimizing revenue during the transition.
With the right RCM partner like BillingParadise, you’ll move into 2026 ready – reducing risk, boosting revenue, and turning industry changes into opportunities.
Frequently Asked Questions





{kind=link}
{kind=link}