


Table of contents
When bundled payment models were first introduced in orthopedics, many of the providers viewed them cautiously. They sounded promising in theory; align incentives, improve coordination, reduce waste; but the real question was whether they would work in day-to-day practice.
Over time, what became clear is that orthopedics is uniquely suited for episode-based reimbursement. The clinical pathways are relatively standardized, outcomes are measurable, and costs are predictable enough to manage; if the right infrastructure is in place.
According to the AHIP Measurement Effort survey, nearly 45% of U.S. healthcare payments now flow through advanced alternative payment models, including bundled payments that hold providers accountable for quality and cost outcomes rather than volume alone.
But not all bundled payment models operate the same way. The details matter.
The Bundled Payment Models Most Suitable for Orthopedics
1. Comprehensive Care for Joint Replacement (CJR)
CJR is launched by CMS, focused specifically on lower extremity joint replacements, primarily total hip and total knee arthroplasty. What made it different was that it was mandatory for selected hospitals, which meant organizations had to adapt quickly.
Here’s how it worked:
CMS established a target price for each hospital based on historical spending and regional benchmarks.
The episode began with hospital admission for joint replacement.
It extended 90 days post-discharge.
All Medicare Part A and Part B spending during that period was included; hospital services, physician services, post-acute care, readmissions, and more.
At the end of the performance year, CMS reconciled actual spending against the target price. If the hospital came in below the benchmark and met quality thresholds, it could receive a reconciliation payment. If it exceeded the target, repayment was required.
In practice, CJR exposed something many organizations hadn’t fully appreciated: post-acute care was the biggest driver of variation. Skilled nursing facility utilization, length of stay, and readmissions significantly influenced performance.
Hospitals that built strong preferred post-acute networks, standardized discharge pathways, and closely monitored 90-day outcomes tended to perform best.
CJR wasn’t just a payment model; it forced hospitals to build episode management capabilities that many didn’t previously have.
2. BPCI Advanced
BPCI Advanced gave organizations more strategic flexibility. Unlike CJR, participation was voluntary. Providers including hospitals and physician group practices could select specific clinical episodes to participate in. Orthopedic episodes commonly included:
- Major joint replacement of the lower extremity
- Spine surgery
- Hip and femur procedures
- Fracture care
BPCI Advanced also used a 90-day episode window and retrospective reconciliation against a target price. However, target pricing methodology was more dynamic and adjusted for patient complexity and regional variation.
A 2022 JAMA study of nearly 4.8 million Medicare episodes found that hospitals participating in the CMS BPCI-Advanced bundled payment program realized an average reduction of roughly $175 per episode and an aggregate savings of about $75 million across the first two model years, highlighting the potential for episode-based models to lower overall spending compared with traditional fee-for-service care.
One of the key differences in BPCI Advanced is physician engagement. Because physician group practices could participate directly, surgeons had stronger incentives to understand the cost drivers of episodes of care payment. This often led to:
- Standardized implant selection discussions
- Evidence-based post-acute referral patterns
- More active monitoring of complications and readmissions
BPCI Advanced rewarded data fluency. Organizations that invested in analytics, tracking cost by discharge destination, by surgeon, by complication profile, were better positioned to manage risk.
It shifted orthopedic leaders from simply delivering surgery to managing performance across the full episode.
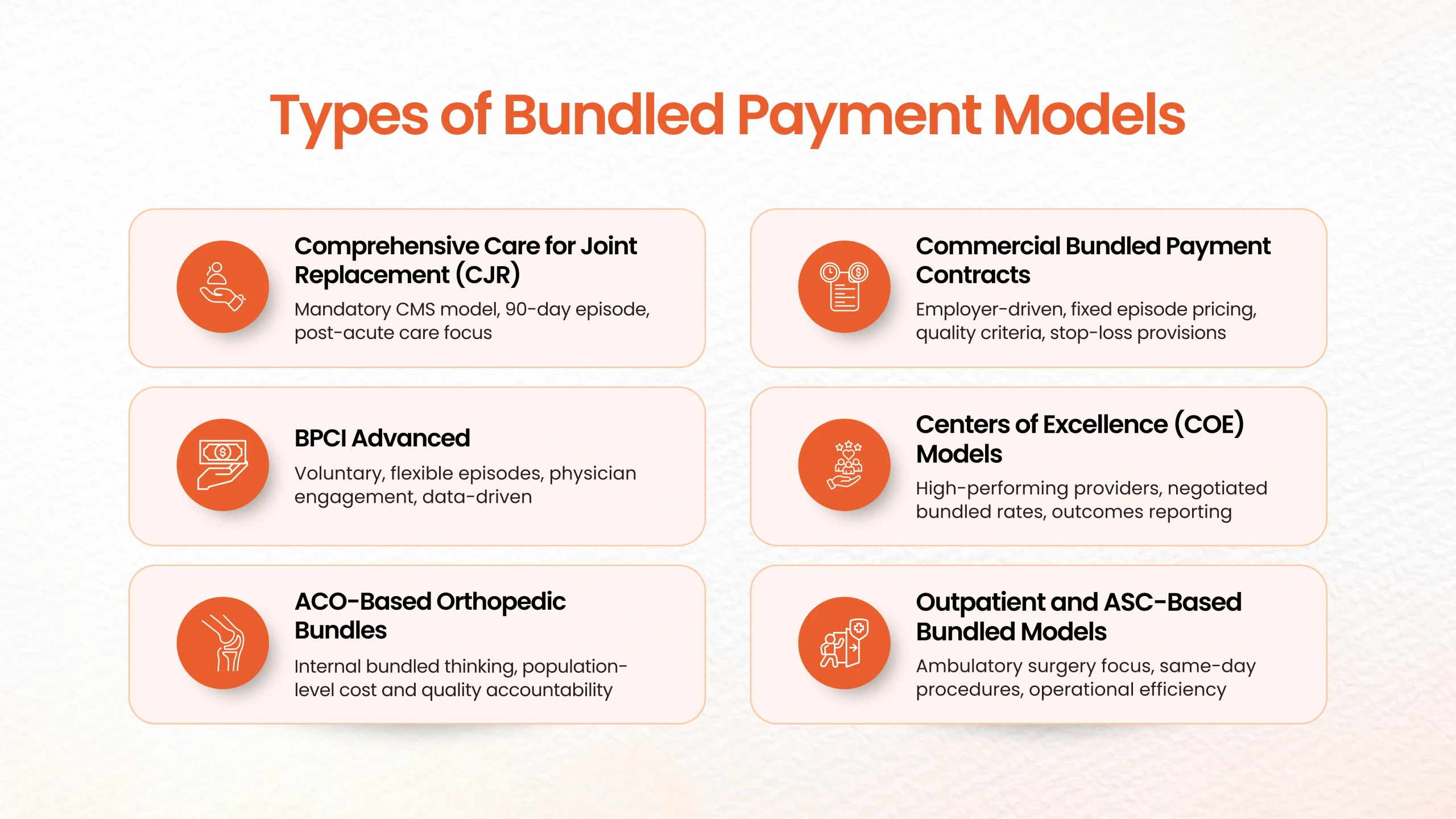
3. Orthopedic Bundles Within ACO Structures
In Accountable Care Organizations, bundled payment principles show up in a slightly different form.
ACOs are responsible for total cost of care across a population, not just a single episode. But because joint replacements and spine procedures represent significant spending, orthopedic care often becomes a strategic focus area.
In this context, episode management isn’t always tied to a formal bundle contract. Instead, systems apply bundled thinking internally:
- Are surgical indications consistent and appropriate?
- Are patients optimized pre-operatively?
- Is discharge to home being maximized when safe?
- Are readmissions being actively tracked and prevented?
Orthopedic optimization becomes a lever for improving shared savings performance at the population level.
What changes operationally is that orthopedic departments become more integrated into system-wide cost and quality strategy; not isolated service lines.
“For many participants, the biggest advantage of the bundled payment initiative is its accessibility. For years, physicians and hospitals have experimented with risk-based payments and value-based service delivery. Accountable care organizations, physician-hospital organizations and especially co-management arrangements were built to deliver on these promises. This initiative offers hospitals a substantial opportunity to capitalize on the work they have done and the relationships they have built in taking a true first step toward fee-for-value care.”
- Jim Bonnette, MD, Chief Medical Officer, Oliver Wyman
4. Commercial Bundled Payment Contracts
Commercial payers and self-funded employers have taken the core principles of CMS models and adapted them.
These bundles often feature:
- Prospectively negotiated fixed episode prices
- Defined quality performance criteria
- Clear inclusion and exclusion rules for services
- Stop-loss provisions for high-risk outliers
Some contracts include warranties, for example, covering certain complications or readmissions within a defined timeframe at no additional cost.
What makes commercial bundles distinct is their market orientation. Employers want predictability. They want transparency. They want high-performing providers.
This has led to more rigorous outcomes reporting, tighter pathway standardization, and stronger emphasis on patient experience. In many markets, bundled contracts have become part of competitive differentiation.
5. Centers of Excellence (COE) Models
Centers of Excellence arrangements are perhaps the most refined version of orthopedic bundled payments.
In these models:
- Employers or third-party administrators select high-performing orthopedic providers.
- A bundled rate is negotiated for defined procedures.
- Travel benefits and care navigation are often included.
- Outcomes reporting is typically required.
COE bundles frequently include total hip replacement, total knee replacement, and complex spine procedures.
From a provider perspective, these models require strong internal discipline. Complication rates, length of stay, discharge disposition, and patient satisfaction must be consistently high. There is little room for unmanaged variation.
COE participation often signals that a program has matured in its ability to manage the full episode; clinically, operationally, and financially.
6. Outpatient and ASC-Based Bundled Models
As more orthopedic procedures move into ambulatory surgery centers (ASCs), bundled payment models are adapting.
Same-day joint replacement is becoming increasingly common. Arthroscopy and outpatient spine surgery are frequently structured under fixed episode pricing arrangements.
In outpatient bundles, the cost structure changes, but the accountability remains:
- Pre-operative optimization still matters.
- Post-discharge monitoring is still critical.
- Complications can quickly erase margins.
What differs is the tighter margin environment. Outpatient bundles require precise operational efficiency.
The Common Thread Across All Models
Despite structural differences, all orthopedic bundled payment models share core elements:
- A defined episode window (often 90 days).
- A target or negotiated price.
- Quality metrics tied to financial performance.
- Retrospective reconciliation or prospective pricing.
- Accountability for post-acute outcomes.
Success under any of these models comes down to three capabilities:
- Data transparency
- Post-acute network alignment
- Surgeon engagement
Bundled payments don’t automatically improve care. They expose variation. What organizations do with that visibility determines whether they succeed.
Orthopedics has become one of the clearest demonstrations that when episodes are defined and managed intentionally, value-based reimbursement can work.
And increasingly, it’s not a question of whether bundled payment models will shape orthopedic care.
It’s how prepared each organization is to operate within them.
Practical Challenges Providers Face Under Fee-for-Service in Orthopedics
Fee-for-service has shaped orthopedic care for decades. For many organizations, it built strong surgical programs, supported procedural growth, and created a clear structure for how services were delivered and reimbursed.
There’s a familiarity to it. You perform a service, you bill for it, you’re reimbursed for it.
But as orthopedic care has evolved, with more emphasis on recovery outcomes, outpatient expansion, and coordinated care journeys, some practical limitations of fee-for-service have become more noticeable.
Most of these challenges aren’t about clinical quality. They’re about structure. The system is built around individual services, while orthopedic care increasingly functions as a connected episode.
That tension shows up in several ways.
Orthopedic Care Rarely Fits Into a Single Billable Event
Anyone who works in orthopedics knows that a joint replacement or spine surgery is not just a procedure. It’s a journey.
There’s pre-operative optimization. Patient education. Surgical planning. The operation itself. Post-discharge follow-up. Rehabilitation. Monitoring for complications. Recovery support that can stretch for weeks or months.
Under fee-for-service, each of those touchpoints is billed separately. On paper, that makes sense. In practice, it can make the care experience feel segmented financially, even when clinical teams are trying to manage it as one continuous process.
Providers often think in terms of episodes. The reimbursement model thinks in terms of encounters.
That disconnect can make coordination more difficult than it needs to be.
Preventive and Recovery Work Isn’t Always Fully Supported
Some of the most important work in orthopedics happens outside the operating room.
Pre-surgical optimization such as managing diabetes, addressing obesity, improving strength before surgery can significantly reduce complications. Clear discharge planning and mobility education can prevent readmissions. Ongoing recovery check-ins can catch problems early.
These efforts take time and coordination. They improve outcomes.
But in a fee-for-service structure, preventive conversations, care coordination calls, and recovery oversight are not always reimbursed consistently or adequately. Providers may invest heavily in them because they know they matter, not because the payment model strongly supports them.
Over time, that misalignment becomes more visible.
Administrative Complexity Is More Demanding Than It Appears
From the outside, fee-for-service sounds simple: deliver care, submit a claim, receive payment.
In orthopedic practice, it’s rarely that straightforward.
A single orthopedic episode can involve:
- Multiple ICD-10 diagnosis codes
- CPT procedure coding
- HCPCS supply and implant reporting
- Payer-specific modifiers
- Distinct documentation requirements
When you add in multiple providers and care settings, hospital, ambulatory surgery center, therapy clinics, imaging centers, the administrative coordination becomes significant.
Even well-managed orthopedic programs devote considerable resources to coding review, denial management, prior authorizations, and reimbursement follow-up. That workload doesn’t directly improve clinical care, but it’s necessary to sustain operations under fee-for-service.
Over time, administrative burden becomes a meaningful operational consideration.
Post-Acute Cost Variation Is Hard to Influence
One of the realities in orthopedics is that what happens after surgery often drives a large portion of total cost.
Skilled nursing facility stays, extended rehab utilization, and unplanned readmissions can significantly impact overall spending.
Under fee-for-service, these downstream services are reimbursed separately. That structure can make it more difficult for orthopedic providers to influence total episode cost, even when they are working to standardize discharge planning or build preferred post-acute networks.
Providers may focus intensely on surgical efficiency and implant selection, yet still see variation emerge in the post-discharge phase, an area where financial accountability is often distributed across multiple entities.
Innovation Doesn’t Always Fit Neatly Into Traditional Billing
Orthopedic care is changing. Many programs now use telehealth follow-ups, remote monitoring tools, digital physical therapy platforms, and nurse navigators who proactively guide patients through recovery.
These innovations improve access and continuity. Patients appreciate them. Clinically, they make sense.
But reimbursement policies can vary significantly. Some virtual services are reimbursed inconsistently. Preventive or coordination-focused efforts may not align clearly with traditional billing structures.
This can slow the adoption or scaling of care models that are designed around patient experience rather than visit-based billing.
Revenue Predictability Can Be Fragmented Across the Episode
In a high-volume orthopedic program, revenue is tied to individual claims. Payment timing varies by payer, denials occur, patient responsibility fluctuates and authorizations can delay care.
When care spans multiple settings, inpatient, outpatient, therapy, follow-up, forecasting full-episode financial performance becomes complex.
You may know the expected reimbursement for a procedure. But predicting the financial picture for the entire recovery journey requires piecing together multiple moving parts.
As orthopedic programs grow and expand into outpatient settings, that variability becomes more noticeable at the enterprise level.
A Structural Tension, Not a Clinical One
None of these challenges suggest that fee-for-service cannot support high-quality orthopedic care. It has done so for decades.
But as orthopedics becomes more outcome-driven, recovery-focused, and coordinated across settings, the limitations of a service-by-service reimbursement structure become clearer.
Providers are increasingly managing episodes.
The payment system, in many cases, is still managing encounters.
That gap is what has fueled interest in bundled payment models, and why many orthopedic leaders are now asking a different question:
If care is delivered as an episode, should reimbursement reflect that reality?
Let’s explore that next.
Fee-for-Service vs Bundled Payments in Orthopedics
What’s becoming clear is that Epic is no longer viewed as just an EHR. For many hospitals and health systems, it’s a strategic platform for scaling operations, managing acquisitions, and stabilizing revenue in an increasingly difficult financial environment.
| Category | Fee-for-Service Model | Bundled Payment Model |
| Payment Structure | Separate payment for each service | Single payment for full orthopedic episode |
| Incentive Focus | Volume of services delivered | Value, outcomes, and efficiency |
| Revenue Predictability | Variable, claim-dependent | More stable, episode-based |
| Administrative Burden | High multiple claims, denials | Lower consolidated episode billing |
| Post-Acute Spending | Often increases due to separate billing | Reduced through care coordination bundled payments |
| Complication Impact | May generate more billable services | Increases episode cost, incentivizing prevention |
| Patient Experience | Fragmented care + surprise bills | More coordinated and transparent |
| Quality Accountability | Limited episode-level accountability | Strong focus on outcomes and performance |
Despite the critical role of comprehensive and team-based care in improving health outcomes, primary care, the backbone of preventive and coordinated care, accounted for only about 4% of total U.S. health spending in 2022, dipping even lower within Medicare fee-for-service populations. Meanwhile, over 40% of healthcare payments in 2023 remained purely fee-for-service, a structure that continues to reward discrete services rather than the coordinated care patients truly need.
So what makes bundled payments so beneficial in orthopedics? Let’s explore through the most important provider-focused questions.


Key Benefits of Bundled Payment Models in Orthopedics
-
Financial Predictability & Revenue Stability
How would bundled payments improve the provider’s ability to forecast revenue compared to fee-for-service?
Under fee-for-service, orthopedic revenue depends heavily on service volume and claim-by-claim reimbursement. Even within the same procedure type, payment outcomes can vary due to payer rules, denials, and post-acute billing complexity.
Bundled payments introduce greater predictability by defining the reimbursement for the full episode upfront.
That allows orthopedic organizations to:
- Forecast revenue per surgical case more consistently
- Plan staffing and implant utilization more strategically
- Reduce uncertainty tied to fragmented billing
Instead of relying on multiple claims being paid correctly, bundled models create a clearer financial structure across the entire episode.
Would a fixed episode payment reduce reimbursement uncertainty and payer variability?
Yes; and this is one of the biggest operational advantages.
In fee-for-service, an orthopedic episode generates dozens of separate payments, often involving:
- Facility billing
- Surgeon billing
- Imaging services
- Anesthesia claims
- Post-acute rehab claims
Each carries its own reimbursement risk.
Bundled payments in healthcare reduce this variability by consolidating reimbursement into one episode-based payment, which can significantly improve payment consistency and reduce payer-related surprises.
How can bundled models protect margins as orthopedic procedure costs rise?
Orthopedic care is becoming more expensive due to:
- Higher implant costs
- Labor shortages
- Increased outpatient surgical volumes
- Rising post-acute care spending
Fee-for-service doesn’t inherently reward cost efficiency; more services often mean more reimbursement.
Bundled payments, however, encourage providers to manage the total cost of care while maintaining outcomes.
A large scoping review of orthopedic bundled payment programs found they were commonly associated with lower episode spending without worsening outcomes.
That margin protection is especially important for high-cost procedures like total joint replacement.
What financial upside exists if we deliver care below the target bundle price?
Bundled payments create a meaningful incentive that fee-for-service lacks: shared savings opportunities.
If an orthopedic provider delivers the full episode efficiently; while meeting quality benchmarks; they may retain savings when costs fall below the target price.
In contrast, under fee-for-service:
- Providing fewer services typically reduces revenue
- Preventing complications doesn’t necessarily create financial upside
Bundled payments reward orthopedic programs for doing what value-based care intends: delivering better outcomes with smarter resource use.
-
Total Cost of Care & Efficiency Gains
How do bundled payments in healthcare help us reduce unnecessary post-acute care spending?
Post-acute care is one of the biggest cost drivers in orthopedic episodes, especially after joint replacement.
In fee-for-service, post-acute utilization often increases because every additional rehab visit or facility stay generates separate reimbursement.
Bundled payments encourage more appropriate discharge planning, such as:
- Avoiding unnecessary skilled nursing stays
- Using home-based rehab when clinically appropriate
- Reducing extended post-acute episodes
Research shows much of the savings in orthopedic bundles comes specifically from reductions in post-acute care spending.
What cost drivers can we control better under bundles?
Bundled payments in healthcare shift focus from isolated services to episode-wide performance.
Orthopedic teams gain stronger control over:
- Avoidable readmissions
- Surgical site infections
- Implant variation
- Length of stay
- Rehab intensity
In fee-for-service, complications may actually increase reimbursement through additional services.
In bundled care, complications increase episode cost and reduce performance; creating stronger incentives for prevention.
Can bundled payments encourage smarter resource utilization without compromising outcomes?
Yes, and that balance is why orthopedics is considered one of the best specialties for bundled care.
Evidence suggests bundled payment models reduce spending while maintaining similar or improved quality outcomes compared with fee-for-service.
That means providers can reduce waste without reducing care quality—a major advantage in today’s reimbursement environment.
-
Reduced Administrative Burden
Would bundled payments simplify billing compared to managing multiple claims under fee-for-service?
Fee-for-service orthopedic episodes create complex billing workflows, with separate claims across multiple providers and settings.
Bundled payments streamline reimbursement by reducing fragmentation.
This can mean:
- Fewer individual claims
- Less reconciliation effort
- Lower denial volume
- Clearer episode-based payment tracking
This administrative simplification is a major operational advantage for orthopedic revenue cycle teams.
How much staff time could we save by reducing claim fragmentation and denials?
Under fee-for-service, RCM teams spend significant time managing:
- Coding edits
- Denial appeals
- Payer follow-ups
- Payment mismatches
Bundled payments reduce these burdens by consolidating reimbursement into episode-level structures, allowing staff to focus more on analytics and performance improvement rather than claim firefighting.
Can episode-based reimbursement reduce payer disputes and authorization complexity?
Because bundled arrangements define episode expectations upfront, they often reduce disputes over individual line items.
While prior authorization may still exist, bundled models can minimize repeated payer challenges around post-acute services, readmissions, or rehab billing.
-
Quality of Care & Outcomes Improvement
Do bundled payment models incentivize better surgical outcomes than fee-for-service?
Fee-for-service rewards volume. Bundled payments reward value.
That means orthopedic teams are incentivized to improve:
- Pre-surgical optimization
- Standardized clinical pathways
- Post-op recovery adherence
- Complication prevention
CMS highlights quality improvement payment models as a core purpose of bundled payment models.
How can bundled payments reduce complications, avoidable readmissions, or revision surgeries?
Complications are costly under bundled models.
That motivates providers to invest in:
- Infection prevention protocols
- Patient risk stratification
- Strong rehab coordination
- Follow-up engagement
Evidence supports that orthopedic bundles often lower spending without harming outcomes, suggesting better complication management.
What clinical quality metrics will matter most under orthopedic bundles?
Common orthopedic bundle metrics include:
- Readmission rates
- Complication frequency
- Length of stay
- Patient-reported outcomes
- Total episode cost
These measures align reimbursement with real performance rather than service quantity.
-
Patient-Centered Care & Experience
How do bundled payments create a more seamless and transparent experience for orthopedic patients?
Fee-for-service often results in multiple bills and disjointed care coordination.
Bundled payments support:
Better episode navigation
Clearer cost expectations
Coordinated recovery pathways
This improves patient confidence and satisfaction throughout the orthopedic journey.
Could bundles reduce surprise billing and improve cost clarity for patients?
Yes. Bundled structures create a more consolidated view of cost, reducing the fragmented billing experience common in fee-for-service episodes.
How Bundled Payments Address Patient Expectations Around Predictable Surgical Costs?
One of the biggest shifts in orthopedics isn’t just clinical, it’s financial. Patients increasingly want to know, upfront, what their surgery is going to cost.
Under fee-for-service, that’s difficult to answer clearly. A joint replacement can generate separate bills from the surgeon, the hospital or ASC, anesthesia, imaging, physical therapy, and sometimes post-acute facilities.
Even when care is well coordinated clinically, the billing experience can feel fragmented. Patients often don’t see the full financial picture until weeks after the procedure.
Bundled payments in healthcare change that dynamic.
Because the episode is structured around a defined package of services, typically covering the surgery and a 30- to 90-day recovery window, it becomes much easier to have a straightforward pricing conversation at the beginning of the journey. The services are viewed as one coordinated episode of care, not a string of unrelated transactions.
From an operational standpoint, that supports:
- Clearer upfront cost estimates
- Fewer unexpected billing surprises
- A more streamlined financial experience
For orthopedic organizations, this matters. Patients, employers, and payers are all prioritizing affordability and transparency. When providers can speak confidently about the total episode of care payment, not just the procedure fee, it builds trust.
In today’s environment, predictable pricing isn’t just a financial feature. It’s part of the overall patient experience.
So, What Does the Bundled Payment Future Mean for Orthopedics?
The future of orthopedic reimbursement is not going to revolve around volume alone. It’s going to revolve around how reliably you can deliver outcomes across the full 30-, 60-, or 90-day recovery window; clinically and financially.
Bundled payments simply make that expectation explicit.
Orthopedic organizations should focus on:
- Standardizing pathways where evidence is clear
- Being intentional about post-acute utilization
- Investing in care navigation
- Measuring complication and readmission drivers
- Understanding your true episode-level margin
The organizations that will lead in the next five to ten years are not necessarily the ones doing the most cases. They’re the ones delivering the most consistent recoveries with the clearest financial accountability.
For orthopedic groups, willing to embrace that discipline, bundled payments are less a threat and more an opportunity – to strengthen payer partnerships, differentiate in the employer market, and build a musculoskeletal program that is both clinically excellent and financially durable.
The question isn’t whether bundled models will continue to expand. It’s whether your organization will be ready when they do.





{kind=link}
{kind=link}